Meaningful weight and hunger reductions in children and adults

In patients 6 years and older with obesity due to POMC, PCSK1, or LEPR deficiency
IMCIVREE delivered significant and clinically meaningful weight loss1
- POMC or PCSK1 deficiency: 80% of patients achieved a ≥10% weight loss from baseline after 1 year (95% CI: 44.4%, 97.5%; P<0.0001; N=10)1,2
- LEPR deficiency: 45.5% of patients achieved a ≥10% weight loss from baseline after 1 year (95% CI: 16.8%, 76.6%; P=0.0002; N=11)1,2
IMCIVREE was studied in 2 identically designed, 1-year, open-label studies, each with an 8-week, double-blind withdrawal period in patients 6 years and older with obesity due to POMC, PCSK1, or LEPR deficiency.1,2
POMC/PCSK1 Deficiency: Mean Percent Change in Body Weight Over 1 Year (n=9)*,1
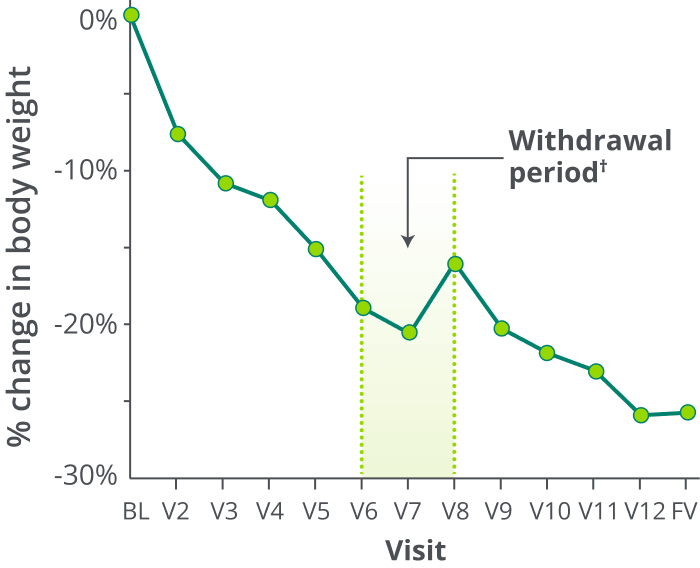
23.1% mean reduction
in weight from baseline
after 1 year (95% CI: -31.9%, -14.4%;
P=0.0003; N=10)
Weight increased during the withdrawal period, then decreased once treatment was reinitiated†
*Participants who achieved weight loss threshold (≥5 kg or 5% if baseline body weight was <100 kg) during the 10-week open-label period.1
†The withdrawal period lasted 8 weeks, which included 4 weeks of IMCIVREE followed by 4 weeks of placebo.1
LEPR Deficiency: Mean Percent Change in Body Weight Over 1 Year (n=7)*,1
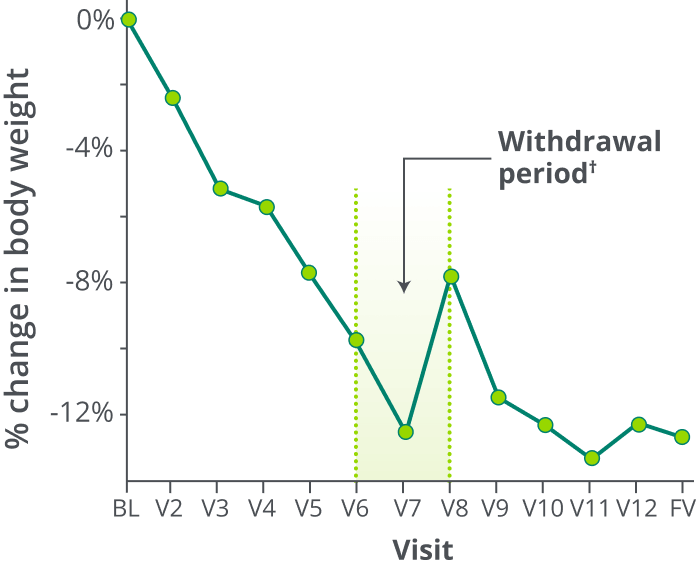
9.7% mean reduction
in weight from baseline
after 1 year (95% CI: -16%, -3.3%;
P=0.0074; N=11)
Weight increased during the withdrawal period, then decreased once treatment was reinitiated†
*Participants who achieved weight loss threshold (≥5 kg or 5% if baseline body weight was <100 kg) during the 10-week open-label period.1
†The withdrawal period lasted 8 weeks, which included 4 weeks of IMCIVREE followed by 4 weeks of placebo.1
In patients 12 years and older with obesity due to POMC, PCSK1, or LEPR deficiency
IMCIVREE decreased hunger over 1 year1
2-point reduction
in median hunger score for POMC or PCSK1 deficiency
In patients with obesity due to POMC or PCSK1 deficiency (n=8), IMCIVREE demonstrated a median 2-point reduction in maximal hunger score at 1 year (Range: -6.5, -0.1)
3.4-point reduction
in median hunger score for LEPR deficiency
In patients with obesity due to LEPR deficiency (n=8), IMCIVREE demonstrated a median 3.4-point reduction in maximal hunger score at 1 year (Range: -4.7, 1.0)
When treatment was withdrawn, hunger scores generally worsened and then improved when IMCIVREE was reinitiated.1
I’m very satisfied. I've lost a lot of weight, and I have a lot more energy. It's nice to see that someone is paying attention to this, and there’s a medication.
– Person who is living with POMC deficiency
A lot has changed. Today, my hunger is, I assume, on the same level as other people.
– Person who is living with POMC deficiency
Individual results may vary.
Get your patient started with IMCIVREE.
See efficacy data for IMCIVREE in young children.
CI=confidence interval, LEPR=leptin receptor, MC4R=melanocortin-4 receptor, PCSK1=proprotein convertase subtilisin/kexin type 1, POMC=proopiomelanocortin.